Epiglottitis is a rare life threatening upper airway infection. The acute bacterial infection of supraglottic structures presents as rapidly progressing stridor, and may result in severe airway obstruction. Epiglottitis requires immediate advanced airway management.
Classification
Upper airway infections are common pediatric illnesses. Many illnesses in children present fever, sore throat and dysphagia, including tonsillitis, laryngitis, epiglottitis, aspiration of a foreign body, tracheitis, laryngeal diphtheria and croup. Epiglottitis is rare, and marked by stridor, unlike tonsillitis and laryngitis. Croup is a more common cause of stridor, and generally presents gradually, with low-grade fever and a stereotypical barky cough that is responsive to steroid therapy. Laryngeal diphtheria has largely been eliminated by vaccination, but this rare clinical finding evolves more insidiously with web occlusion of the airway. The airway compromise of epiglottitis progresses rapidly, and children will sit propped forward on their arms to optimize air flow, with drooling as they are unable to otherwise clear oral secretions. Epiglottitis is marked by toxemia with high fever. Cough is not generally seen. Tracheitis may present similarly to epiglottitis and may require rigid bronchoscopy to differentiate the two. Bacterial tracheitis carries a significant mortality rate as high as 40%, while prompt intervention in epiglottis provides a definitive rescue.
Incidence
The incidence of pediatric epiglottitis has fallen substantially with the introduction of the Haemophilus influenzae type b (Hib) vaccine in 1985, to less than 1 case per 100000 mean annual incidence. Hib related epiglottitis was predominately seen in children ages 2 to 6 years. However, a multi-year retrospective review completed in 2006 now identifies a higher incidence in infants < 1year, with 34% of cases having occurred in this group. Another case series completed in 2006 identified bacterial tracheitis, another rare entity, as 3 times more likely to cause respiratory failure than epiglottitis and croup combined, highlighting the rarity of presentation.
Pathophysiology
Acute epiglottitis involves the lingular surface of the epiglottis, the aryepiglottic folds and the arytenoids. With the decrease in incidence of Haemophilus influenzae type b, group A B-hemolytic Streptococci is now the more common bacterial cause of epiglottitis. Other pathogens include Streptococcus pneumoniae, Staphylococcus aureus and Klebsiella pneumoniae. Epiglottitis may manifest as a negative reaction to chemotherapy or super-imposed Candida infection in the immunosuppressed. Acute inhalational injury and chemical burns may also precipitate epiglottitis, with illicit inhalation of cocaine associated with severe presentation.
Clinical Presentation and Diagnosis
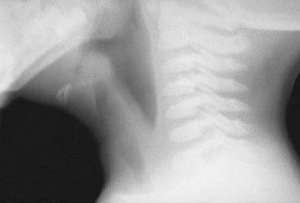
Soft-tissue lateral neck radiograph reveals edema of epiglottis consistent with acute epiglottitis.(https://emedicine.medscape.com/article/763612-overview)Children with epiglottitis appear toxic and present with high fever, odynophagia with a thick, muffled voice, and stridor. Children with epiglottitis refuse oral intake, and will drool rather than swallow oral secretions. Classically, the four D's are described, dysphagia, dysphonia, dyspnea ad drooling. The stridor associated with epiglottitis may be present in other childhood acute upper airway infections, croup among the most common. Epiglottitis is distinguished by its rapid progression, with severe airway obstruction evolving within 6 to 12 hours. As the severity progresses, the child may refuse to lie down, and lean forward using the upper extremities in a tripod fashion, thrusting the chin forward optimize airflow. The inspiratory phase will be marked by obstructive stridor.
Historically, epiglottitis was a clinical diagnosis based on presenting symptoms, but with decreasing incidence, it may be less readily recognized. Cervical neck anterior posterior and lateral films will show a hallmark thumb-sign of the epiglottis on the lateral film, while croup is characterized by a steeple sign on anterior view. Bacterial tracheitis may share characteristics of both croup and epiglottitis, with less definitive findings on imaging but similar rapid progression to airway distress as seen in epiglottitis. Bacterial tracheitis may require diagnostic bronchoscopy to visualize the thick purulent secretions, edema and associated plaques with possible pseudo-membrane formation. However, diagnostic evaluation prior to prompt airway management may risk airway loss as minimal stimulation in both epiglottitis and bacterial tracheitis can devolve into severe airway compromise.
Preoperative Evaluation and Therapy
Epiglottitis is a true airway emergency. While a pertinent history and evaluation is recommended, the urgency of establishing a secure airway must take precedence. Limiting anxiety provoking procedures is encouraged, however, establishing intravenous access prior to anesthesia is critical. An anesthetic plan may involve parental presence at induction to limit patient agitation, but parents must be educated as to the severity of airway compromise expected during this period including the risk of cardiovascular collapse. Heliox therapy may be of significant benefit facilitating care in the emergency room and transporting to the operating room, as the helium component improves linear airflow and reduces respiratory work. Hi-flow may also be beneficial.
Laboratory studies are not considered diagnostic for epiglottitis but viral serology may help clarify clinical course. Surface cultures obtained at the time of airway examination may also help delineate bacterial etiology and guide antibiotic therapy if indicated.
An otolaryngologist ideally is actively engaged throughout, with a plan to support anesthesia services with rigid bronchoscopy, suspension laryngoscopy and possible emergent tracheostomy if needed.
Anesthetic Management
An advanced difficult airway setup is recommended prior to induction of anesthesia, including various laryngoscope blades, LMAs, multiple ETT sizes, video laryngoscopy and fiberoptic bronchoscopy. Visualization of airway structures will be obscured by the engorged epiglottis, challenging both direct laryngoscopy and video laryngoscopy. An age-appropriate endotracheal tube likely will meet significant resistance due to edematous changes, and smaller sizes are typically required.
Mask induction in the sitting position is recommended, with cautious titration of intravenous sedative as needed to deepen the anesthetic plane without suppressing spontaneous ventilation. Muscle relaxation is generally avoided, as the loss of airway tone may cause complete airway obstruction that cannot be rescued by positive pressure ventilation. Airway examination will show a swollen cherry red epiglottitis, and manual chest compressions may be required to elicit bubbles at the glottic opening to identify the airway.
Intensive care management will be required until the airway edema resolves Definitive intravenous access is recommended, with either two peripheral IVs or PICC access to maintain sedation needs postoperatively. Steroid administration is of benefit, and has been shown to reduce the length of ICU admission in adults. Edema resolution may be measured by leak test at the bedside or more formally by airway examination under anesthesia.
Morbidity/Mortality
With the advent of the Haemophilus influenzae type b (Hib) vaccine, the incidence of epiglottitis and its attendant risk of morbidity and mortality declined substantially. Epiglottitis can be associated with epiglottic abscess, with extension to the mediastinal structures described. Drainage of the mediastinum may be needed if necrotizing mediastinitis evolves. These complications may require long-term ventilation strategies and/or tracheostomy.
References
This is a Stub Notice. This page has not been completed. You can work on this page by signing in and going to the Edit tab. Thanks for helping to make PedsAnesthesia.Net Wiki useful.